Kentucky's child welfare watchdog says the system has 'a culture of secrecy'

– 13 min read

Kentucky's State Auditor says the state failed Miya Rudd- and that only one person has the power to force real change.
"I'm Shay McAlister, and this is Shay Informed: an independent, ad-free platform dedicated to honest journalism with compassion and clarity.
Are you new here? Sign up for the free weekly newsletter or subscribe to support our mission and access behind-the-scenes content, podcasts, and in-depth stories reserved for paid subscribers.
When I published my investigation into the death of Miya Rudd last month, one of the central questions I couldn't fully answer was this: if the Child Fatality Review Panel can only make recommendations, and the Cabinet for Health and Family Services can simply choose not to follow them- who actually has the power to force change?
I went looking for that answer. It led me to Kentucky State Auditor Allison Ball.
What I found in that conversation was more than I expected. Auditor Ball didn't just confirm what my investigation had found. She expanded it- with information about her own office's battles to access records, a frank assessment of the culture inside the cabinet, and an answer to that central question that names one person, and one person only, as the decision-maker who can force Kentucky's child welfare system to change.
That person is the governor.
I'll get to that. But first, there are some things Auditor Ball told me- and a document her office provided- that I think every Kentuckian needs to see.
Paid subscribers- you can LISTEN to this report now. My new podcast episode covers the case, and my conversation with the auditor. Find that link at the bottom of this page.

When Miya Rudd's death first became public, the Office of the Ombudsman- the oversight body specifically designed to investigate the Cabinet for Health and Family Services- didn't have access to the information it needed.
At the time, the Ombudsman's office was still housed within CHFS itself, which created an obvious conflict of interest. When Auditor Ball brought the office under her authority, she expected to inherit the data access that came with it. Specifically, access to iTWIST- the state's case management database that contains records on every child involved with DCBS-Department of Community Based Services- Kentucky's CPS branch.
The Cabinet said no.
"The Ombudsman had historically always had access to iTWIST, but that access was turned off when it was switched over to the auditor's office," Ball told me. "We had several meetings and tried to get access to it, and we weren't able to reach an agreement."
So the office that is legally charged with overseeing Kentucky's child welfare system had to file a lawsuit against that system to see CPS records.
They won. Through a settlement, Ball's office now has access to iTWIST- and Miya Rudd's case was specifically cited as the reason they needed it.
"We referred to Baby Miya's death as a reason why we needed to have access to it," Ball said. "It's helpful to have a concrete example, and unfortunately, hers was a very good example of why we needed to have access."
Let that sit for a moment. An oversight body had to take the Cabinet to court to do its job. And a dead eight-month-old was the argument they used to win.

Readers of my original investigation will remember that the Cabinet for Health and Family Services refused to answer multiple specific questions I submitted before publication- including whether anything had changed after Miya's death and whether workers would face retaliation for speaking with me. Their response to four direct questions was a statement that didn't address a single one of them.
When I described that sequence to Auditor Ball, she wasn't surprised.
"We have legal authority to be able to have access to information, and we also have trouble getting information from the Cabinet for Health and Family Services," she told me. "Your experience is in line with our experience. There is a culture of secrecy, I think, over there, and it's very difficult to get information."
The state's own oversight office- with legal authority and subpoena power-describes the Cabinet for Health and Family Services as operating with a culture of secrecy. That is not my characterization. It is the characterization of the elected official whose job it is to keep the cabinet accountable.
Ball was careful to acknowledge that some of what the Cabinet protects is legitimately confidential- locations of children, personal identifying information. But she drew a clear line between appropriate confidentiality and what she's seen in practice.
"When you get very vague answers or very general answers, it just leads to uncertainty that they're doing what they're supposed to do," she said. "There is a way to make sure there's accountability. There's still a way to make sure the public is informed. And unfortunately, when you get vague answers, that's not being achieved."

Once Ball's office gained access to iTWIST, they began doing something they called deeper dives- focused investigations into specific patterns of failure rather than broad, surface-level audits of the entire cabinet.
Child fatalities became one of those deeper dives. They hired a retired Kentucky State Police detective specifically to focus on cases involving children who died while interacting with the system- someone who, as Ball put it, "knows what leads to a child fatality and what we need to be looking for."
What they found was not reassuring.
"The breakdowns that you've mentioned- those are breakdowns that even with the access that we have, we've been able to see recurring in other child fatality instances," Ball told me.
She specifically highlighted a documentation failure that went beyond what I had reported. "Documents don't often show up until months later," she said. "You can have a child fatality and three months later the documents show up in iTWIST showing what the progress was in that case. That raises all kinds of concerns. You don't know when those documents were created. You don't know how accurate they are."
And worse: she said her office has reviewed multiple cases that had partial documentation, or no documentation at all.
I now have a document that shows exactly what this looked like in Miya's case.
The Ombudsman's office provided me with the Corrective Action Plan (CAP) issued in connection with her case. What it reveals goes beyond what appeared in the state's own report- and it raises new questions about the integrity of the records that now exist in iTWIST about what happened to her.
The Office of the Ombudsman issued the CAP on June 24, 2024. Ten days after Miya's body was found.
The complaint that triggered it had been received by the Ombudsman's office on June 17, 2024. Three days after her remains were discovered.
The Ombudsman determined the complaint was justified on three grounds: service recordings did not reflect all contact attempts or attempts to locate the family before the case was closed on February 21, 2024. The only documentation was a vague notation that "multiple attempts were made"- with no dates. The safety plan completion was not documented in service recordings. And there was no record of who was supervising contact between the child and the mother.
In other words: the file that existed for Miya's case showed almost nothing about what had actually happened during the search for her.
On June 26, 2024- twelve days after Miya's body was found- the supervisor on the case sat down and entered all of the missing contacts into iTWIST. Using the caseworker's handwritten notes, because the caseworker was on leave, according to the CAP.
The records about what happened during the search for Miya Rudd were being written- and entered into the state's official system- after she was already dead.
This is precisely what Auditor Ball described to me. Documents appearing months after events they were supposed to record. No way to verify when they were created. No way to verify how accurate they are.
Now there is a specific document proving it happened in Miya's case.
But the CAP reveals something else. Something that doesn't appear in the state's SARS report. That's the report workers create after a child fatality.
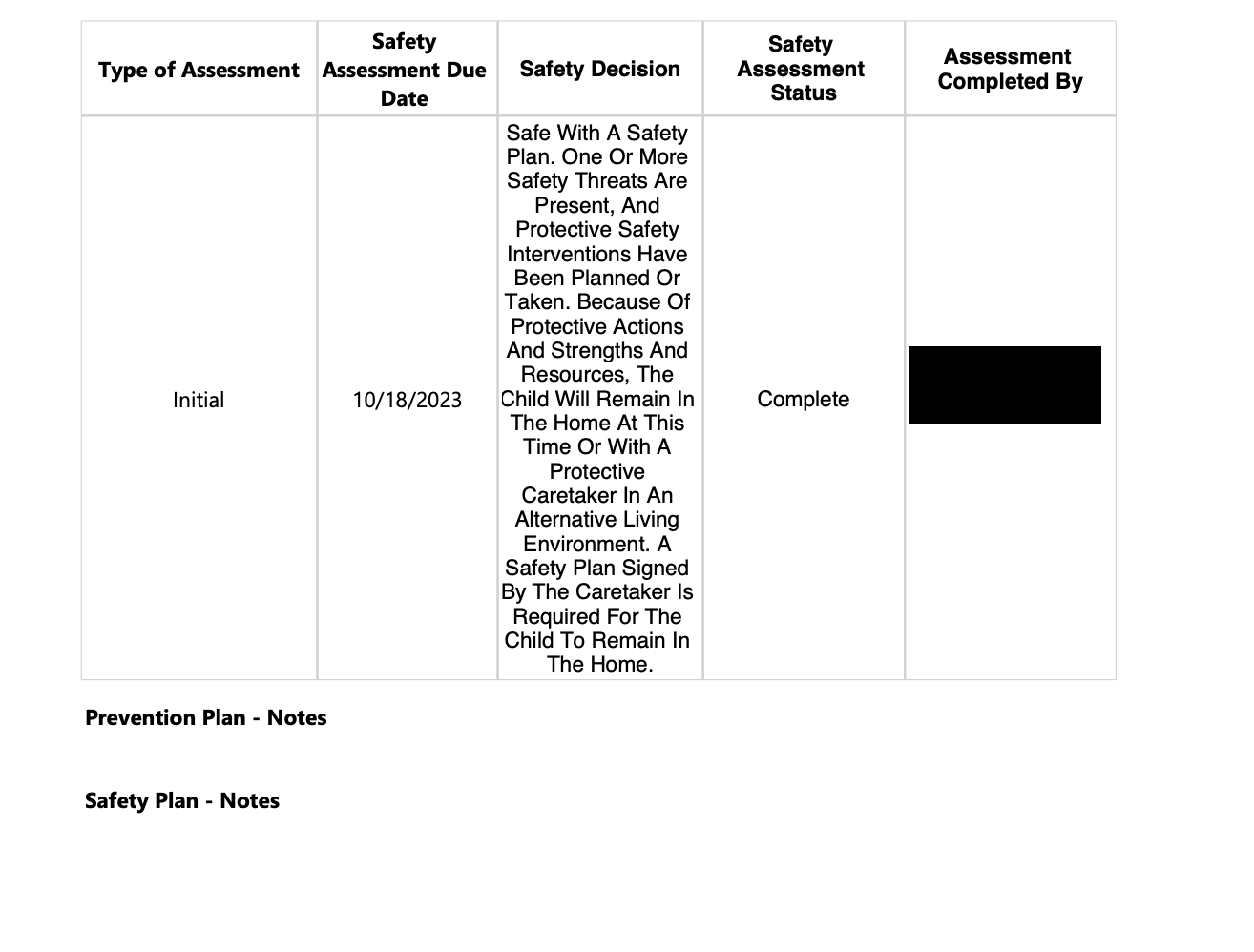
The CAP states: "Although the safety plan uploaded in iTWIST states 'signed in person' it should have stated 'verbally agreed.'"
The SARS report describes a handwritten safety plan that was accidentally shredded and replaced with a generic version. But this document reveals that the plan actually uploaded to iTWIST was recorded as "signed in person" when it was only verbally agreed to over the phone.
That is two separate documentation failures on the same safety plan. The original was destroyed. And the replacement record was inaccurate about how the agreement was even reached.
Auditor Ball explained the Corrective Action Plan process to me in our interview. The cabinet is required to respond. Required to document what steps they took. Required to explain what they will do to prevent the same failure from happening again.
Here is what the response to Miya's CAP said.
Regional administrators held meetings. Teams calls were conducted. An email was sent to the supervisor and a regional coordinator about how a CAP works and providing a link to a Standard of Practice document. The missing contacts were entered into iTWIST. And the policy violation would be discussed at a staff meeting.
To prevent this from happening again: supervisors will talk with their teams to ensure service recordings are detailed and properly entered. Supervisors will review service recordings and send them back to workers if information is missing.
That is the corrective action for a case that ended with an eight-month-old found dead in a duffle bag.
A reminder to document better.
There is no mention in the CAP response of caseload conditions. No mention of the absence of law enforcement contact during 45 days of searching for a missing infant. No mention of a gap in training on what to do when a newborn that screened positive for meth goes missing.
The state identified one failure- inadequate documentation- and the fix was a staff meeting reminder and a link to a policy document.
The SARS report identified four learning points. The corrective action addressed one. Partially.
When I asked whether what happened to Miya was an aberration or a pattern, she confirmed what I feared- that her office has seen similar breakdowns repeatedly across multiple child fatality cases. But then she described something specific that her office has encountered in their investigations. An attitude.
"There's been an attitude from supervisors that, 'Well, you know, this is a family that has problems, so if we don't do a good job here, if we forget to file a document, it's okay, because they're just going to be back again, and we can address it later.'"
That phrase- they're just going to be back again- is a version of the same logic documented in the SARS report on Miya's case. Workers and supervisors believed that closing the file on a repeat client was acceptable because another referral would eventually come in. The mother was a repeat client. Something else would come in.
The CAP document makes that attitude visible in a new way. The records that were supposed to document what happened during the search for Miya didn't exist until after she was dead. They were created- by her supervisor, from handwritten notes- after her body was found. As if the documentation could be completed later. As if there would always be more time.
There wasn't.
"In Baby Miya's case, there wasn't another time. Because she had died. And that just underscores the importance of doing it right the first time. Don't have the attitude that you're going to get a second chance. You may not get a second chance," she said.
I asked Auditor Ball directly. I wanted it on the record from the person whose office exists to hold this cabinet accountable.
"Do you believe the cabinet and the state of Kentucky as a whole failed this baby?"
Her answer was immediate. "Oh, I do. I really do."
She went on: "It's one of the reasons why I'm in the job that I'm in. Because I believe that there are children like Baby Miya all over the Commonwealth of Kentucky that need to be protected. And my job is to make sure the cabinet is doing what it's supposed to do."
She told me that within her office, Miya is referred to by name. That she and a few other children have become what Ball described as sources of motivation- children who are named in meetings, children whose cases remind the staff why the work matters.
"She's a beautiful baby," Ball said. "And she should definitely still be here."
Auditor Ball's office has real authority that the Child Fatality Review Panel does not. She has subpoena power. She can impose Corrective Action Plans that the cabinet is legally required to respond to. She can make findings public.
A CAP was in fact issued in Miya's case. I now have that document.
The cabinet responded. And that response- a staff meeting, a reminder to document better, a link to a policy page- is the accountability that exists on paper for what happened to Miya Rudd.
When I asked Ball whether her office could actually compel the cabinet to change- not just respond, but actually change- the answer carried a limitation she was candid about.
"Other than the CAP, which does have an accountability mechanism to it- we don't have a lot of teeth," Ball acknowledged. "We can't impose fines. We can't put somebody in jail. There aren't a lot of tools to enforce and make sure that people are doing what they're supposed to do."
A required response is not the same as required action. And a corrective action plan whose fix is a staff meeting reminder has consequences that are, ultimately, reputational rather than legal.
Which brings me to what I consider the most important exchange in our entire conversation.
I told Ball what Dr. Melissa Currie had told me- that the Child Fatality Review Panel has no statutory authority to compel anyone to act. I told her that from the outside, it seemed like every oversight mechanism in Kentucky was advisory. That findings could be issued and recommendations made, but nothing could ultimately be forced.
I asked: does anyone have the power to force change?
"Yes, absolutely," Ball said. "You have to remember- this is a governor's cabinet. The governor is your primary person who's tasked with dealing with these situations. He hires and fires the people that he appoints, can set policies and training and requirements in place. Ultimately these kinds of fixes happen when you have leadership who does the right thing. And that's the governor. The governor's appointees. That's your ultimate decision maker, right there."
I pushed. I wanted to make sure I was hearing her correctly.
"So at the end of the day, the governor is the only one who's in a position today to to force a change", I asked her.
"Yes," she said. "Yes. I think that's the most accurate way to say that."
The child fatality panel makes recommendations. The auditor makes recommendations and can impose corrective action plans. The legislature can call hearings and pass laws. But the Cabinet for Health and Family Services is the governor's cabinet. The people running it serve at his pleasure. The policies governing how Kentucky's social workers operate- what they're trained to do, what tools they have, what caseloads they carry- are ultimately set and enforced by people who answer to one person.
Governor Andy Beshear.
I have requested an interview with the governor's office. As of Monday morning, I have not heard back.
Ball's office is continuing its investigation into child fatalities in Kentucky- including Miya's case. She told me they have done all they can with the information currently available to them, but that they are working to gain access to additional records, including autopsy reports and complete police investigations, that they don't yet have.
She ended our conversation with a message for the public: the Office of the Ombudsman exists, it is independent from the cabinet, it protects confidentiality absolutely, and it wants to hear from Kentuckians who have concerns about how the Cabinet for Health and Family Services is treating people in its care.
"If people have a concern, we're here," Ball said. "We want to listen. You can provide a tip, and we will make sure it stays confidential."
The number for the Kentucky Office of the Ombudsman is 1-800-372-2973. You can also submit a complaint online at auditor.ky.gov.
This story is available to LISTEN to at the link below. Paid subscribers have full access to all of my podcasts, wherever you like to listen! Just click on "One More Question" and follow the steps you see below.